Red Medicine: Socialized Health in Soviet Russia
IT IS desirable to give a preliminary statement on public health administration and especially on the evidence which vital statistics give as to health conditions, before describing the general conditions of clinical work in Russia. In actual fact public health administration is in so large a measure combined with clinical work that the two cannot be logically separated.
Throughout our inquiry we have regarded the entire framework of Russian society as involved in any inquiry into medical work in Russia; for national health is a function of society, and the normality of other aspects of communal life has an influence on health not less than that of medical care. It is for this reason we have brought into our review, as factors of health, the conditions of industry and agriculture, housing, home life, marriage and divorce, and social insurance.
Several chapters have already been devoted to the physiological side of special health work, including the activities of infant consultations, of child centres, of creches and kindergartens, and of prenatal consultations and maternity homes and hospitals. In one chapter we have already stepped over the dividing line between physiology and pathology in discussing intentional abortion, which has momentous social as well as medical importance.
The framework of public health administration is identical with that of general medical administration. The entire practice of medicine, institutional and domiciliary, having been socialized, is supervised and controlled by the public health organization in each of the seven constituent republics. In this respect, as also in the main in actual working, there is no separation between clinical and preventive medicine. Each doctor is expected to consider the health of his patient, not merely as a patient, but as a member of the community, whose efficiency, if possible, must be increased.
The organization of the public health and medical service is centralized in each of the seven constituent republics, but there is no central All-Union department of health. exceptions, however, are that the health service in the Army and Navy and for the railroad workers is administered by All-Union authorities. While the seven People's Commissariats of Public Health and their subordinate organizations are politically independent of one another, the system established in the R.S.F.S.R., with the seat in Moscow, in most respects serves as a model for the other six. The scope of each of the seven commissariats includes administration of preventive medicine, medical care, pharmacy, medical training; and of certain health resorts not under control of the social insurance system.
Subordinate to the Commissariat of a constituent republic are District and Regional Branch Commissariats. There are also Special Commissariats in the cities.
Each of the seven People's Commissars is appointed by the Presidium, a committee representing the Tsik, another committee; which in turn represents the Congress of Soviets. Heads of the District or Regional Commissariats are appointed by District Committees. The Commissar of Health of the republic is entitled to nominate a candidate, and although the local Committee chooses him, the centrally nominated candidate is seldom rejected. The Commissar may also veto a local nomination. The only difference of opinion likely to arise is as to qualifications. An official can be dismissed either by a local or the central committee.
We may cite one or two examples of how the State and local authorities cooperate. In Kharkov special committees of institutions and of local authorities nominate candidates, and these are appointed if approved by the Commissar of Health of the Ukraine. Even in large factories, such as the Tractor Works, the final medical appointments rest with the Commissar, who can also remove unsuitable persons from their posts.
In Tiflis we were informed that local authorities recommend candidates for special local posts. These, if endorsed by the Commissar of Health for Georgia, become valid; if not, a more appropriate appointment must be made. The local body can appeal against this decision to the governing body of Georgia.
If a doctor does his work well, he is reappointed. Political considerations are stated not to weigh in the
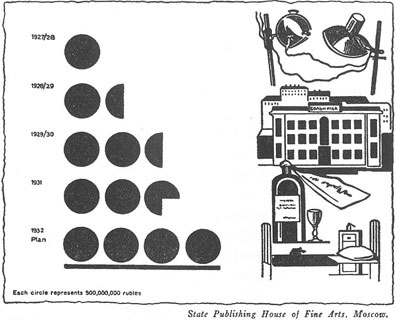
Fig:4. Growth of public health appropriations in the Union of Soviet Socialist Republics since 1927-1928. The figures for 1932 are estimated.
appointments, and in fact 70 per cent of the medical officers in the employment of the Republic of Georgia are non-Party men. The desire for efficiency on every side is said to be such that Party considerations and favoritism have no chance.
The preceding statements apply to appointments both for clinical and special public health posts.
The people generally are stated to take unusual interest in public health administration, and our observations confirmed this claim.
The general principle of medical organization is that of a chain of controlling bodies each closely related to the other. There are "flying squads" of officials through whom it is possible to concentrate on places in which serious needs arise, especially in areas in which great construction works are in progress.
In each constituent republic of the Soviet Union and in its chief divisions a few doctors are always available for special public health work; but in each district the local doctor is expected to supervise health conditions as well as to treat the sick. This is true also in the medical administration of large factories, the physicians of which are more engaged in hygienic work and in the regulation of the medical care of workers than in actually undertaking this care.
The detailed organization of general medical and health work in the Ukraine may be outlined as an example. This outline is based on an interview with Dr. Kantorovitch, Commissar of Health of the Ukraine:
The heads of each special department form the Collegium at which points of policy are discussed. The chief departments are concerned with :
1. Therapeutics.
2. Medical work in institutions (dispensaries, hospitals, etc.) . This section has many inspectors and subinspectors.
3. Care of mothers and children.
The last section cares for kindergartens, nurseries, and mothers' consultations, and prepares the staff for their work and nurses for work in the nurseries of collective farms, etc. Last year 57,000 women were prepared for this work.
4. Industrial hygiene, factory doctors, etc.
5. The betterment of children's health, school hygiene, etc.
6. Sanitary conditions of life:
(a) Feeding and nutrition.
(b) Housing.
(c) Water, sewage, etc.
(d) Epidemiology and prevention of infections.
7. Scientific research.
Arrangements are made for technical instructions of workers, for correspondence classes, and for encouraging scientific research at polyclinics. Fiftytwo scientific institutions come within this division's supervision.
8. Popular sanitary education.
Much work of this kind is done by university professors, and special courses of one or two years have been organized. Persons having gone through these courses are often invited to become social workers in the centres of medical work.
9. Rationalization.
Problems are given to the several institutes for study and the suggestion of remedial measures.
10. Planning department, including finance and statistics.
11. Supply department for food, etc., and for maintenance of institutions.
12. Division for plans of buildings.
Local budgets are framed by the local Executive Committee, and then submitted to the Ukraine Central Government, which may send them back for revision. They finally require to be approved by the People's Commissars of the Republic.
The financial needs of social and medical work are met from three sources, namely:
1. Local taxes used for supporting local institutions.
2. Central funds contributed especially for maintenance of medical and other staff.
3. Insurance funds from which most of the money needed is derived.
This expenditure is solely for insured persons and their families, which form a great majority of the total population.
In the following pages are given some of the chief vital statistics of the U.S.S.R. They have been abstracted chiefly from the International Health Year-Book, published by the Health Section of the League of Nations.
In 1929 the population of the U.S.S.R. is estimated to have been 157,611,ooo as compared with 39,607,000 for England and Wales and 120,000,000 for the United States.(1)
Russia's industrial population in 1929-30 is given as 10,887,000 as compared with 8,886,ooo two years earlier, an increase in this short interval of 22.8 per cent as compared with an increase of 2.2 per cent of the total population in the same interval.
The International Health Year-Book for 193o gives the birth rate in 1929 in the R.S.F.S.R. (European territories) as 38.6 per 1,000 of population, while the death rate was 20.6. In the rural population the birth rate was 41.4, in the urban population, 28.4. The following figures for some Russian cities are given:
| BIRTH RATES | DEATH RATES | ||
| 1913 | 1929 | 1929 | |
| Moscow | 32.2 | 22.0 | 13.2 |
| Leningrad | 26.4 | 22.1 | 15.4 |
| Kharkov | 46.5 | 19.1 | 11.8 |
| Rostov | 22.3 | 13.8 | |
| Saratov | 24.6 | 18.8 | |
Infant mortality rates form a sensitive index of domestic sanitation and of personal hygiene and care, and, assuming that registration of birth and deaths is fairly accurate, the following figures are important.
In European Russia the infant mortality rate per 1,000 births in 1913 was 275; in 1927 it was 186, annd in 1930 it was 141.
In 1929 the infant mortality rate was in Moscow 131; Kharkov 106; Leningrad 151; Rostov 146; and Saratov 178.
Evidently, although infant mortality remains excessive, there has been a marked reduction in it, which indicates a great improvement in personal hygiene since the Revolution.
The following additional figures from the same source are useful indices of public health in Russia. Those of England and Wales are given in a parallel column for rough comparison, and the two can be compared by remembering that the population of the U.S.S.R. is about four times that of England and Wales. The figures for England and Wales are approximately complete; it is likely that those for Russia are not equally so.
| CASES OF ACUTE INFECTIOUS DISEASES IN 1929 | ||
| U.S.S.R. | England and Wales | |
| Smallpox | 6,099 | 10,967 |
| Scarlet Fever | 458,704 | 120,232 |
| Diphtheria | 98,565 | 62,774 |
| Dysentery* | 177,252 | 573 |
| Typhoid Fever* | 171,263 | 2,835 |
| Typhus* | 33,127 | 1 |
| Relapsing Fever | 2,939 | 0 |
| Malaria | 2,993,072 | 0 |
As bearing on domestic cleanliness and communal sanitation, the figures for the items marked* have special significance.
The figures for relapsing and typhus fevers are important indices of intense overcrowding and personal hygiene and of social backwardness. So also are the figures for trachoma, of which there were 1,146,599 cases in the Union, chiefly in the more remote and primitive parts. The fact that there is fifteen times as much typhoid fever in Russia as in England for equal units of population shows the need for great reforms in municipal and communal sanitation, as regards water supplies and other sources of infection.
(1) The population of the United States according to the census of 1930 was 122,775,000.