Ian Burge Archive | ETOL Main Page
From Militant, No. 348, 25 March 1977, p. 5.
Transcribed by Iain Dalton.
Marked up by Einde O’Callaghan for the Encyclopaedia of Trotskyism On-Line (ETOL).
From the General Household Survey interviews, men of working age in the professional classes reported losing, on average, fewer than four working days a year, whereas unskilled manual workers reported losing more than eighteen days annually. If the whole of the male working population had had a sickness absence rate equivalent to that reported by the professional classes there would be an annual saving of about 100 million working days.
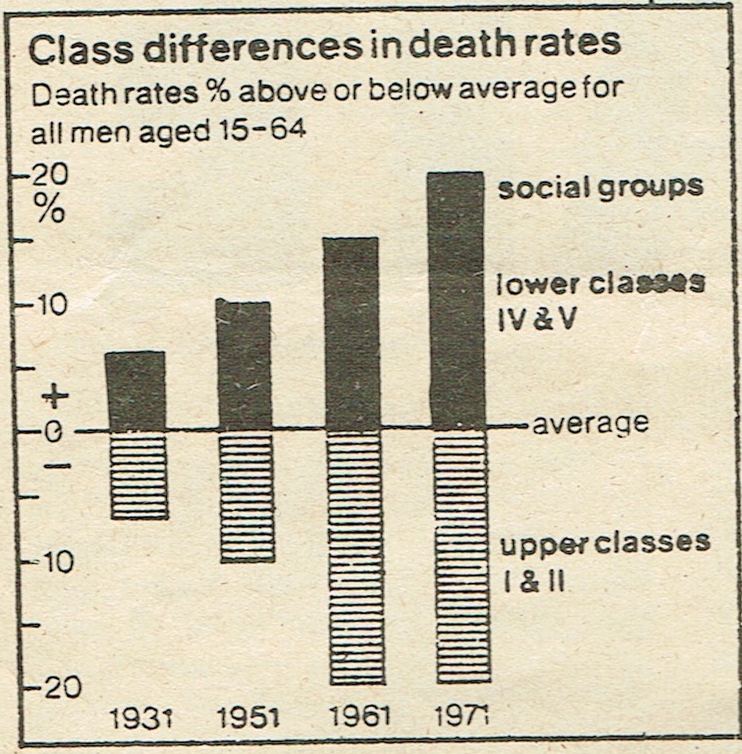
Unskilled manual workers and their families suffer two or three times more than senior professional and managerial families from almost all the major causes of premature death, and the overall death rate is now 50% higher in the bottom quarter of the population than the top quarter. This means that the working class generally are considerably more susceptible to early death than the middle and upper classes.
These differences between the social classes is two or three times as large now as it was during the 1930s and 1940s (see chart). Although the illustration is based on the figures for males, working class women suffer a worse health record than do middle class women.
|
|
Women aged 15 to 64 years whose husbands were in the professional groups were subject to a death rate (adjusted for age) 35% below the national average while women whose husbands were in unskilled occupations had a mortality 66% above the professional figure. This shows that disparities cannot be attributed to employment factors alone. The working class mother is more than twice as likely to die from complications during pregnancy and birth as her middle class counterpart.
One of the health measures most strongly reflecting the general living standards is the infant mortality rates. Here again there are tremendous differences to de found in different areas, for example Bromley, a middle class southern suburb of London, has an infant mortality rate of 12.4 in a thousand. Lambeth however, a few miles away and working class, has a rate of 20.8.
Perinatal mortality, that is the number of deaths at birth or during the first few days of life, per thousand deliveries, is 28.9 in Tameside, Manchester, and 13.2 in Oxfordshire. The national figure is about 19, compared with Sweden’s 12.
The Court committee’s report on Child Health Care, published last December, noted that “twice as many children of unskilled workers die in the first month of life as children of professional workers, and the gap between the social classes in this respect has been widening steadily for 25 years.” Some causes of infant death, such as gastroenteritis and pneumonia, are five times more prevalent in the working class than in the higher social classes.
The working of the present Abortion Act leads to many anomalies.
In some areas it is easier than others to obtain an NHS abortion. But
there is no area where all abortions are done on the NHS. Relying on
private or charitable agencies discriminates against the working
class woman.
Thus we see that the working class suffers a relatively greater need for the services, in terms of its propensity to illness, yet at the same time is relatively under-provided, as revealed by the following examples:
A comparison between the working class area of East London with Essex gives you a clear picture of inequality. The infant mortality rate is 50% higher in E. London than in Essex. In 1974 the notification rate for TB in E. London was three times the national average and over seven times the rate for Essex. And it is getting worse. Between 1967 and 1974 respiratory TB increased in E. London by 50% and no-respiratory TB doubled.
The poor health of the working class compared to the middle class is a direct result of the living conditions imposed on us by capitalism. Lack of money to buy sufficient food, fewer holidays, bad working conditions and long working hours, fewer recreation facilities combined with bad housing forced on us by profit-conscious landlords makes a joke of “equality of life” in this class society.
In 1971 overcrowding was 50% worse in E. London than the whole GLC area. 4½ times more E. London households had no fixed bath than those in Essex; three times more had an outside toilet only; and three times more had no continuous hot water. Yet despite greater need for health care, the percentage of GPs there working single handed is almost twice the national average and the percentage of GPs over the age of 60 is also nearly twice the national average. There are only 12.7 health visitors per 100,000 population instead of the 23 recommended for such high risk areas.
A number of government publications have appeared during the last year dealing with the problems of the NHS. A future article in Militant will discuss these in more detail. Their main proposal is that the inadequacies in the services are somehow to be made good by redistributing funds from ‘rich’ areas. There are no ‘rich’ areas. As a matter of fact, the City and East London is designated as a comparatively ‘rich’ area! What the NHS needs as a matter of great urgency is a massive injection of funds to bring up all the services to a decent standard, as far as the working class are concerned.
Ian Burge Archive | ETOL Main Page
Last updated: 11 February 2017